My father spent the last 12 days of his life unconscious, unresponsive, in a hospital bed on Queensland’s Sunshine Coast.
My mother sat beside him night and day, holding his hand. I massaged Dad’s legs, horribly swollen, the effects of oedema – a buildup of fluids. His mouth fell open, dried out; I swabbed it constantly in an attempt to keep it wet. Sometimes his breath was a gurgle. My brother and I took turns sleeping on a stretcher in his room – the “dying room” was what hospital staff called it.
I whispered to him, “You can go now, we love you.” But for 12 days Dad remained tenaciously alive. Had he known of his grievous state, he would not have been happy.
We were distraught. What did he know? Was he frightened? Was he in pain but unable to tell us?
Dying is difficult, a nurse told me – it can be an unmercifully long passage.
It might have been even longer and more appalling had Dad not been clear about his wishes.
Soon after he was diagnosed with prostate cancer in 2005, my father signed a legally binding advance health directive, Queensland’s version of what is known in some other states as an advance care directive. AHDs and ACDs record what a person wants in the event they do not have the capacity to make or communicate decisions about their own healthcare or treatment – say in situations such as my father’s decline into unconsciousness, or as a result of a catastrophic accident.
Dad’s directive said he did not want to receive “life-sustaining” treatments including cardiopulmonary resuscitation, assisted ventilation or artificial nutrition. He wanted to die as swiftly as possible without medical intervention beyond palliative care to keep him comfortable.

We might have felt there was little to be thankful for through those wretched days in the dying room but things could have been much worse.
‘It’s very hard to know which family member you should be listening to’
One day at the nurse’s station outside my father’s room I saw three people arguing with one another and a doctor. It was heated, circular, unpleasant. Decisions about their loved one’s care were up for debate.
At least we knew what Dad wanted. But too few Australians have such certainty: only 33% of Australians have undertaken some form of advance planning and only 6% of them have formally completed an ACD, according to a 2025 study conducted by Advance Care Planning Australia.
When there is no legally binding directive in place, the consequences can be grim: people might receive interventionist treatments they would never have wanted had they been able to express their wishes. Families, meanwhile, can find themselves in dispute about treatment decisions at a time already characterised by enormous stress and anguish.
Associate Prof Davinia Seah, the head of palliative medicine at St Vincent’s hospital in Sydney, frequently sees conflict between family members. “We’ve had situations where one daughter will say, ‘Mum really wanted to be comfortable, let’s just dose her up on morphine’ and the other family member will say, ‘No, I want everything done, they need to be in ICU, they need to be intubated,’” Seah says. “It’s very hard to know which family member you should be listening to because there’s no documentation.”
Seah says people’s manner of death often reflects the way they lived: “If your family has been arguing for many years, unfortunately that’s probably going to manifest itself in someone’s death as well.” (Queensland’s AHD form has space to jot notes under the statement “I would prefer these people not be involved in discussions about my health care.”)
Clinicians, Seah says, are thankful for more harmonious situations in which a family member can speak for their loved one in the absence of written instructions. “It’s really important that they are able to say, for example, ‘Mum said that she never wanted to be hooked up to machines.’”
When there is neither documentation nor a legally appointed “enduring guardian”, doctors like Seah are in the dark. “I’ve got a patient at the moment who has had some mild cognitive impairment and a range of neighbours have been really supportive but no one has actually been appointed to make decisions, so we’ve got to figure out, ‘Are these neighbours trustworthy, are they really thinking of this patient’s best interests?’ That’s a tricky situation to be in.”
If a written document has been completed, she says, it’s vital that it can be produced at the hospital. “Today I had a conversation with an 87-year-old lady who came into hospital with heart problems. She scored a tick – she has an advanced care directive – but when I asked where it was she said it was with her solicitors. Do you know how hard it is to get that paperwork?!”
One doctor who asked not to be named says she has helped her own parents finalise their directives, even though it was a struggle to persuade her mother to think about the future. “Mum is fiercely independent and would rather die than have someone help her shower, for example, but she is still resistant to talking about what might eventually happen,” the doctor says. “I have too often watched older people die in hospitals or be maimed by well-meaning CPR/life-sustaining measures when their wishes are not set out formally.”
‘If this thing fails, just let me go’
John Groves, a New South Wales retiree, completed an ACD after coming close to death multiple times over the past year. “It’s all written down now … what we want done,” he says in a Zoom call from his Port Macquarie lounge room, turning to look at his wife, Dawn, beside him. “Everything’s pretty black and white with us now.”
About 15 years ago, Groves developed cardiomyopathy. By late 2025 his body was failing him. “It all got pretty bad, pretty quick,” he says.
In September, he collapsed at his cardiologist’s office. He was resuscitated and intubated at Port Macquarie base hospital before being airlifted to Sydney. “It was pretty scary,” says Dawn, a social worker and case manager at Kempsey correctional centre.
At St Vincent’s hospital, Groves had a mechanical heart pump surgically implanted but soon afterwards developed a liver infection. He becomes emotional as he talks about the effect of his health crises on his family. “The poor buggers, they’ve been told four or five times now that … I’m probably not going to wake up, it’s pretty tough on them.”
A St Vincent’s palliative care specialist suggested that Groves should complete an ACD. “She would come in and have the discussion with us and then after a couple of visits, she’d leave some paperwork for us to have a look at.”
The decisions John has documented in his ACD reflect his concern for his family. “I was in hospital for four months! I’ve had a million needles and a million tests. It’s a lot. And it’s not just a lot for me, it’s a lot for Dawn.” He points to the external battery pack and controller connected to his heart pump: “If this thing fails, just let me go.”
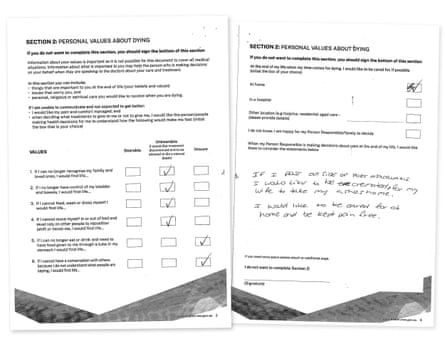
Among the declarations in his ACD, Groves has noted that he wants to be cared for, if possible, at home when he is dying and to be kept pain-free. He would accept resuscitation/CPR but not renal dialysis or “life prolonging treatments that require continuous administration of drug(s)?”. He has recorded that, “If I pass outside of Port Macquarie I would like to be cremated and for my wife to take my ashes home.” He has ticked the yes box in answer to a question about whether he would like to donate his organs and tissues for transplantation after his death.
“I said they could have whatever bits and pieces they wanted but I said to the doctor, ‘I don’t know what you’re going to want because nothing’s any good any more!’”
What makes life worth living?
In addition to recording preferences about treatment, the person you want to make decisions on your behalf and whether you want to donate your organs (which requires additional planning), ACDs typically allow space to outline values that might be relevant at end of life. For example, NSW guidelines suggest people consider stipulating whether they want flowers in their room, to spend time in their garden or for favourite music to be played.
Seah says she has had patients write things in their directives such as “If I can’t eat chocolate, I can’t wipe my bottom, I can’t play golf, life’s not worth living … there’s no point in trying to prolong it.”
I think about what made my father’s life worth living even as he became sicker: being able to enjoy his food, walking to the local shop to buy a newspaper, reading books to his grandchildren. In his last weeks, none of that was possible – and pain became a permanent resident.
And I remember a conversation with a friend who has in place every last possible end-of-life document, from her will to an ACD: “When you don’t have children, when you don’t have a spouse, you really need to get it sorted out.”
On NSW Health’s website I find an advance care directive form. I hit print.